This Alzheimer’s & Brain Awareness Month, we delve into the clinical opportunity of differential diagnosis.
For any patient presenting with the triad, or with cognitive decline where the profile doesn’t quite fit Alzheimer’s, normal pressure hydrocephalus (NPH) deserves systematic evaluation rather than exclusion by default.
The Scale of the Diagnostic Gap
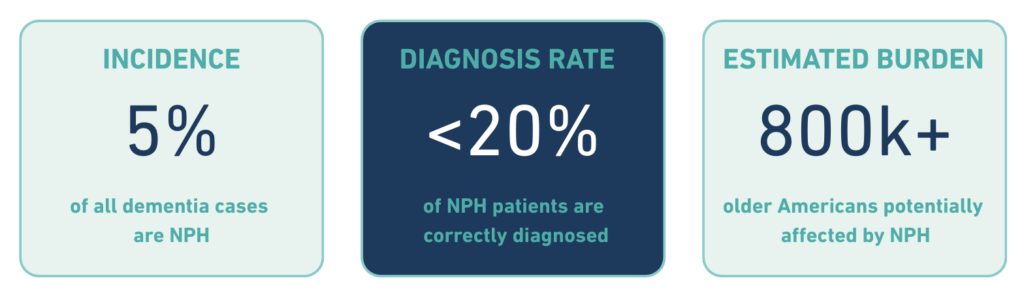
NPH accounts for an estimated 5% of all dementia cases – a meaningful proportion in any memory or falls clinic. Nearly 800,000 older Americans may be living with NPH, yet fewer than 20% of NPH sufferers receive a correct diagnosis.
These figures reflect a systematic failure at the point of differential diagnosis.
Where the Differential Breaks Down
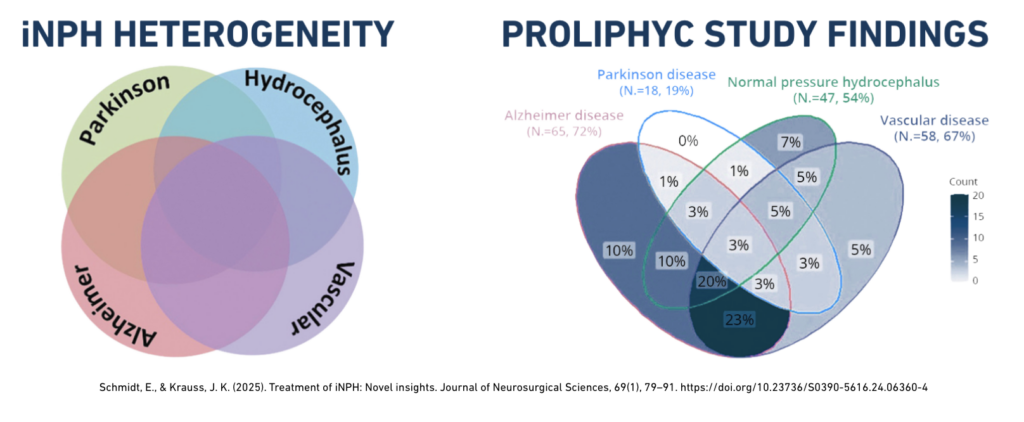
The overlap between NPH and Alzheimer’s disease is well-documented, and it runs deeper than symptom similarity alone. NPH remains a challenging clinical entity with significant overlap in presentation with other neurodegenerative disorders including Alzheimer’s disease, vascular dementia, and parkinsonian syndromes.
Several factors compound the challenge:
- Cognitive profile overlap. NPH-related cognitive impairment (executive dysfunction, psychomotor slowing, and attentional deficits) can be difficult to distinguish from early Alzheimer’s during a bedside assessment. Language and episodic memory are relatively spared in NPH, but this distinction is easily missed without a structured neuropsychological evaluation.
- Gait assessment is inconsistently applied. Gait tends to be affected first and more severely than other domains in NPH, making it the most discriminating early feature in the differential. Yet in practice, a shuffling, magnetic gait in an older patient is often attributed to musculoskeletal causes or general deconditioning.
- Imaging findings are unreliable in isolation. Ventriculomegaly raises suspicion, but cannot distinguish NPH from cerebral atrophy without functional CSF data. The DESH pattern is supportive but not definitive.
- Comorbidity further muddies the picture. The incidence of Alzheimer’s disease in patients with NPH is greater than in the general population, meaning the two conditions genuinely co-exist in a meaningful subset of patients – making clean differentiation harder, but no less important. A concurrent Alzheimer’s pathology does not preclude NPH treatment benefit; it makes accurate identification of the NPH component more, not less, critical.
Unlike Alzheimer’s, NPH Symptoms Can Be Treated
The PENS Trial (NEJM 2025) provides the strongest evidence to date that shunting in correctly identified NPH patients produces clinically meaningful, durable outcomes.
But every participant had already demonstrated CSF-responsiveness via a drainage test prior to randomization. The PENS Trial was not testing shunting in unselected suspected NPH, it was testing it in patients who had been correctly identified through functional CSF assessment. Critically, the treatment effect on NPH symptoms is inseparable from the quality of patient selection upstream.
CSF Infusion Testing as the Differentiating Step
For patients where clinical and imaging findings are ambiguous – which, in the NPH/Alzheimer’s differential, is the majority – objective measurement of CSF outflow resistance (Rout) can provide the functional data that resolves uncertainty. Elevated Rout is not present in Alzheimer’s disease or most other neurodegenerative conditions; it is a marker of impaired CSF absorption specific to the NPH pathophysiology.
The XP One device will bring standardized measurement of Rout to the bedside: a 20-minute outpatient procedure, auto-calibrated for any lumbar puncture needle, delivering real-time CSF data. Our goal is to remove the access and workflow barriers that currently keep most NPH patients from reaching the step on which their improvement depends.
Reach us at contact@x-pressure.com or visit our solutions page to learn more.